Cross-Sectional Analysis of Pyrroles in Psychiatric Disorders
Cross-Sectional Analysis of Pyrroles in
Psychiatric Disorders: Association With
Nutritional and Immunological Markers
Nina Mikirova, PhD
Riordan Clinic, 3100, N Hillside, Wichita, KS, Tel: 316- 927-4753, Email: nmikirova@riordanclinic.org
Abstract Background:
Psychiatrists started using urine pyrroles (hydroxyhemopyrrolin-2-one, HPL)
to diagnose psychiatric disorders many years ago. The biological origins of HPL are not known, nor
are the causes of elevated urinary pyrrole excretion well understood.
Methods: In the present study we analyzed the level of pyrroles in 148 patients with schizophrenia,
135 patients with bipolar disorder, 97 patients with depression, 119 patients with attention deficit
hyperactivity disorder, and compared these data with the results of pyrrole tests for patients with
non-psychiatric conditions and healthy volunteers.
Results: According to our data, urinary pyrrole concentrations tended to be high in patients with
psychiatric disorders, but elevated level of pyrroles was not specific for only these patients. We found
evidence of an allergy related component in the fact that elevated pyrrole levels were significantly
more prevalent in subjects with elevated histamine values. A role of intestinal bacteria, or imbalances in intestinal bacterial metabolism, was also suggested based on the found relationship between
elevated pyrrole levels and elevations in indicans and urobilinogens. In addition, our data demonstrated that subjects with severely elevated pyrrole levels were deficient in nutrients such as zinc,
vitamin B3, and vitamin C.
Conclusion: Thus, pyrrole excretion seems to be a component of illness in general and not strictly
psychiatric disorders.
Background
Interest in pyrroles as markers of psychiatric disorders started Dr. Abram Hoffer’s
discovery that “Mauve Factor”, a pyrrole
named for its lavender appearance in urine
chromatograms stained with Ehrlich’s
reagent,1
was prominent in urine samples
from schizophrenics.2,3 After considerable
efforts,4-10 Mauve Factor was determined to
be the hemopyrrole derivative hydroxyhemopyrrolin-2-one (HPL). Hoffer claimed
that HPL tended to decrease when a patient
recovered from illness, and increased when
illness reappeared; moreover, treatments
with vitamin B6 and zinc were reported to
decrease HPL levels and were associated
with patient recovery.11 Some psychiatrists,
particularly those with interests in orthomolecular medicine, have used HPL as a clinical
tool for diagnosing and following the progression or remission of mental illness.11-17
Data from these studies suggest that roughly
one-third of schizophrenia patients tested
had elevated pyrroles, but high urine HPL
levels were not limited to schizophrenia, as
a variety of conditions and stresses were associated with urine pyrrole excretion.
The biological origins of HPL are not
known, nor are the causes of elevated urinary pyrrole excretion understood. Proposed mechanisms for HPL formation and accumulation in the body include intake from
dietary sources, heme breakdown, or altered
heme biosynthesis, the latter perhaps occurring with the aid of gut flora.18 Irvine has
proposed that HPL is a metabolite of heme
synthesis intermediates porphobilinogen
and prophyrins, as these are structurally very
similar to HPL.9
Increases in pyrrole levels
and excretion may occur as a result of stressinduced changes in intestinal permeability,
which in turn leads to increased pyrrole absorption. To the extent that pyrrole excretion
may be an indicator of heme breakdown due
to emotional stress, oxidative stress, or nutrient deprivation, a study of the correlation
between urinary pyrroles and nutrient levels
should be of interest.
At the Riordan Clinic, urinary pyrrole
measurements have been part of the protocol for diagnosing psychiatric disorders and
other disorders for decades. Access to the
clinic’s database has enabled us to examine
pyrrole levels in patients with a variety of
disorders and to see how they correlate with
the concentrations of other key nutrients
or metabolites. The present manuscript describes our analysis and evaluation of these
data, and provides some assessment of the
potential value of monitoring pyrrole levels
in patients with psychiatric disorders.
Methods
All laboratory tests were conducted by
the Riordan Clinic Bio-Center Laboratory
(Wichita, KS), a licensed and certified medical laboratory (http://www.riordanclinic.
org/laboratory/catalog.pdf ). Handling of
laboratory data by our institute is done in full
compliance with HIPAA regulations. Assay
methods for the various vitamins, minerals,
and lipids for which data are presented here
were conducted by the Bio-Center Laboratory using standard methodologies. Urine
HPL levels was quantified using a colorimetric assay, provided precautions are taken
to keep it stable prior to and during the assay.
Statistical analyses were carried out using the
Excel spreadsheet program and graphs, with
regression data fits where appropriate, were
constructed using the Kalaidagraph program
(Synergy Software, Reading PA).
Inclusionary criteria used were patients
with a diagnosis of psychiatric disorder who
came for treatment at the Riordan Clinic
and had evaluations that included nutritional and pyrrole tests. No other demographic
data except age and sex were recorded for
this study.
The diagnosis of psychiatric disorder was
made by medical doctors using Diagnostic
and Statistical Manual of Mental DisordersIV criteria based on direct observations plus
reports from parents and other care takers.
Results
We analyzed urine pyrrole data in 119
patients with attention deficit hyperactivity disorder (ADHD), 148 patients with
schizophrenia, 135 patients with bipolar disorder and 97 patients with depression. We
initially examined amino acids, key precursors for neurotransmitters. We also investigated other parameters consider relevant to
psychiatric disorders, such as toxic metals,
essential minerals, and fatty acids. Tests for
psychiatric disorder groupings show elevated average values of hair aluminum, lead (in
patients with schizophrenia), iron (total and
hair), arachidonic acid to EPA ratio, omega
3 to omega 6 fatty acid ratios, and urine pyrroles. Deficiencies were found in the levels
of essential metals magnesium, zinc and
copper (serum). Some deficiencies and the
metabolic imbalances in fatty acid, amino
acid, mineral, and pyrrole levels in ADHD
patients were analyzed previously.19
The percentage of patients with increased levels of pyrroles in comparison with
patients without specific diagnosis (134 subjects) is shown in Figure 1 (p.3).
According to these data the percentage
of patients with the levels of pyrroles higher
than 20 ug/dL was 48% for ADHD patients,
22% for patients with schizophrenia, 30%
for patients with bipolar and depression and
26% for patients without specific diagnosis.
Pyrrole distributions in subjects with
illnesses were analyzed by illness category,
along with the distribution that would be
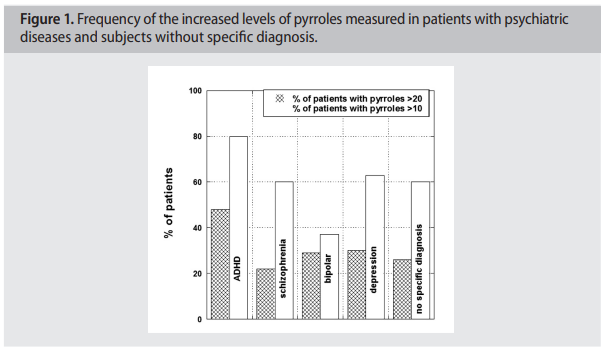
expected if all subjects were in the normal range. There was skew in the data indicating subjects with elevated pyrrole levels in groups of patients with psychiatric disorders. It is particularly acute in ADHD patients, of whom 48% had levels above the normal range. The median of pyrrole values outside the normal range were 47 ng/dL for patients with schizophrenia, 43 ng/dL for patients with bipolar disorder, 39 ng/dL for patients with depression and 44 ng/dL for patients with ADHD. The proportion of subjects with pyrroles outside the normal range was similar to those seen in patients with other illnesses (26 % of all subjects analyzed had pyrrole levels above 20 ug/dL), suggesting that pyrrole levels indicate illness in general and not necessarily psychiatric disorder. To see if pyrrole levels were related to allergic reactions, we compared pyrrole levels with histamine and immunoglobulin levels. For histamine, data are shown in Figure 2 (p.4). There was a statistically significant correlation (p < 0.001) between histamine levels and pyrrole levels, and the vast majority of patients with elevated pyrrole levels showed elevated histamine levels also. For instance, for subjects with histamine levels below 53 ng/dL (the upper limit of normal range in our clinical laboratory), only 16% of subjects had elevated (> 20 ug/dL) pyrrole levels, with only 2% having pyrrole values above 40 ug/ dL and 2% having values above 80 ug/dL. In contrast, 26% of subjects with elevated histamine levels had elevated pyrrole levels, with 9% showing values above 40 ug/dL and 4% showing values above 80 ug/dL. All subjects with pyrrole levels above 100 ug/dL had elevated histamine levels. Similar trends were observed with the immunoglobulins IgM. Relation between IgM and pyrroles is shown in Figure 3 (p.4). For abnormal levels of pyrroles (>20 ug/ dL), 75% of the data showed IgM values higher than 100 mg/dL. The average level of pyrroles was 30 ng/dl ± 8ng/dl for IgM<100 mg/dl, and 46 ng/dl ± 40 ng/dl for IgM>100 mg/dL. Elevated pyrroles are also thought to be related to intestinal issues. The urine indican test is considered an indicator of intestinal toxemia and overgrowth of anaerobic bacteria (indican is a product of bacterial tryptophan digestion), while urobilinogens are products of intestinal bacteria that can build up if the liver is overburdened. Figure 4, (p.5) shows how these parameters vary depending on urinary pyrrole levels. In both
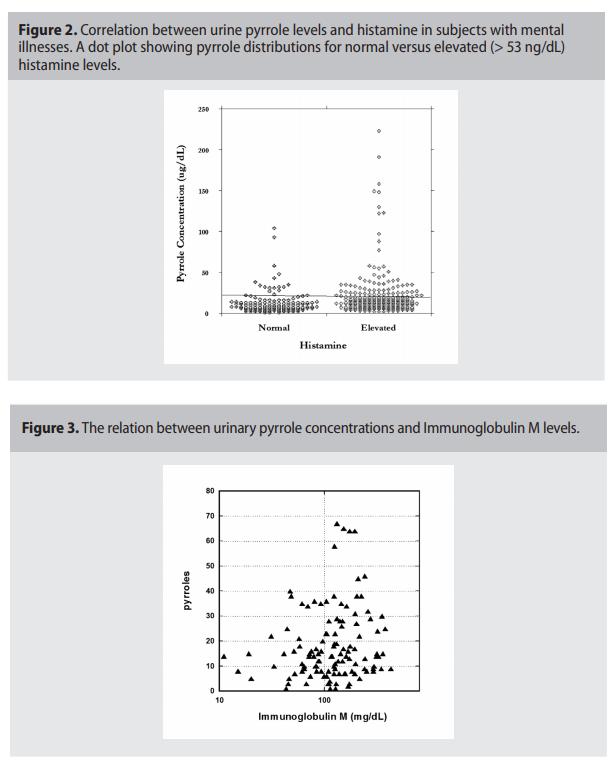
cases, elevated pyrroles were associated with
elevated levels, supporting the hypothesis
that intestinal bacteria overgrowth may be
associated with excessive pyrrole excretion.
To determine if increased pyrroles secretion is accompanied by nutritional deficiencies, we compared urinary pyrrole concentrations with vitamins and minerals in
blood for cases where both were measured
on the same visit. Vitamins are natural barriers against infection and allergic reactions,
as well as chemical balance of essential minerals. Examples of a relationship between
urinary pyrroles and vitamin C or zinc are

shown in Figure 5(a, b).
Vitamin C, vitamin B3, red blood cell
zinc, and zinc to copper ratios were found in
some psychiatric disorder groups to decrease
with increasing pyrrole levels. Examining
Figure 5, it appears that subjects with very
high pyrrole levels (above 40 ug/dL) tended
toward the left hand side of the horizontal
axis, suggesting that data points with very
high pyrrole levels had low nutrient values.
The potential link between nutrient levels
and pyrrole levels deserves further systematic study.
At the Riordan Clinic, patients with
psychiatric disorders are treated by attempting to restore proper mineral balances and correct nutrient deficiencies. We examined
the database for mental illness patients who
underwent this type of therapy (though precise protocol details varied from subject to
subject), compared “initial” to “final” pyrrole
values, and found that pyrrole levels decreased during treatment. We have not yet
conducted a controlled trial where a consistent treatment is used and patient mental
illness (symptom severity) is also monitored
over time.
Discussion
The Riordan Clinic has been measuring
nutrients, minerals, toxins and urine pyrrole
concentrations as a diagnostic tool for over
forty years. In examining laboratory parameters that are thought to be important in
maintaining proper neurological function,
we found several potential trouble signs in
patients with various types of psychiatric
disorders. In particular, the tests demonstrated the elevated average values of aluminum, lead (in patients with schizophrenia),
iron, arachidonic acid to EPA ratio, omega 3
to omega 6 fatty acid ratios, and urine pyrroles. Deficiencies were found in the levels
of essential metals: magnesium RBCs, zinc
RBCs and copper (serum). Urinary pyrrole concentrations also tended to be high
in these patients. We investigated these elevated pyrroles further, finding that nearly
half of the patients diagnosed with ADHD
had pyrrole concentrations above the normal
limit (20 ug/dL) in urine. The proportion was
roughly one-third in subject with depression,
bipolar disorder, or schizophrenia. Interestingly, the elevated level of pyrroles was not
specific for patients exclusively with psychiatric disorders. When we analyzed patients
without psychiatric disorders as a whole (i.e.,
with illnesses ranging from cancer to arthritis, fibromyalgia, and chronic fatigue, among
others) and subjects without specific diagnosis, roughly a quarter of them had elevated
urinary pyrrole levels. Thus, pyrrole excretion
seems to be a component of illness in general and is not strictly associated with psychiatric disorders. We are struck, though, by
how high urine pyrroles can be in mentally
ill subjects, with roughly ten percent having
values above 40 ug/dL and, in the case of
schizophrenics and ADHD sufferers, nearly
5% of subjects having values above 80 ug/
dL. We saw some patients with levels over
200 ug/dL.
Our examination of the Riordan Clinic
database confirms some of the conventional wisdom about pyrrole excretion. We find
evidence of an allergy component in the fact
that elevated pyrrole levels were significantly
more prevalent in subjects with elevated histamine values. Immunoglobulins also appear
to correlate with pyrroles (IgM versus pyrroles).
A role of intestinal bacteria, or imbalances in intestinal bacterial metabolism, is also
suggested based on the relationship between
elevated pyrrole levels and elevations in indicans and urobilinogens. Indicans can be an
indicator of protein digestion efficiency.18
Patients with high urine indicans can be expected to have issues such as insufficient gastric hydrochloric acid, insufficient digestive
enzymes, adverse food reactions, infection,
or bacterial overgrowth. These problems are
also consistent with elevated urobilinogens.
Elevated urine pyrroles, as they correlate
with the other stress factors, may simply be
an indicator of metabolic stress in the body.
It also appears to be a general rule that subjects with severely elevated pyrrole levels
were deficient in nutrients such as nutrients
zinc, vitamin B3, vitamin C. The stress factors described above (infection, toxicity, etc.)
may be factors in causing nutrient deficiency,
or may be caused by nutrient deficiency. Vitamin C in particular is important for innate
and cell mediated immunity, as it protects
neutrophils from oxidative damage. The zinc
to copper ratio is also an indicator of oxidative stress. This redox variable is commonly
outside its normal range in mentally ill subjects, and appears to correlate in some cases
with pyrrole excretion.
At the Riordan Clinic, mentally ill subjects
are treated with supplements (including injections of B-vitamins, and intravenous infusions
of vitamin C) to replenish depleted nutrient
stores and support healthy (normal) immune
function. We were interested to determine
how these treatments affected pyrrole levels.
While we have not conducted a rigorous clinical study in this regard, we were able to extract
from the database a group of subjects who
had similar treatments and for whom pyrrole
analyses before and after extended treatment
was available. The results seem to suggest that
pyrrole concentrations are reduced after prolonged supplementation therapy. This may be
an interesting topic to explore with more rigorous controlled studies.
In summary, our analysis of the Riordan
Clinic patient database suggests that pyroluria is relevant to a variety of stress and illness
conditions. Abnormal pyrrole excretion appears to be an indicator of oxidative stress,
infection, intoxication, or improper digestion.
Competing Interests
The author declares that she has no
competing interests.
References
1. Irvine, DG: Apparently non-indolic Ehrlich-positive substances related to mental illness. J Neuropsychiat, 1961; 2: 292-305.
2. Hoffer A, Osmond H: Malvaria: a new psychiatric
disease. Actapsychiat Scand, 1963; 39: 335-336.
3. Hoffer A: The presence of malvaria in some mentally retarded children. Am J Ment Defic, Def,
1963; 67: 730-732.
4. Irvine DG, Bayne W, Miyashita H, et al: Identification of kryptopyrrole in human urine and its
relation to psychosis. Nature (London), 1969; 224:
811-813.
5. Irvine DG: Mauve factor and 6-sulfatoxy skatole: two biochemical abnormalities associated
with specific measures of psychiatric disease. Clin
Chem, 1963; 9: 444-445.
6. Irvine DG, Bayne W, Miyashita H: The main
form of naturally-occurring kryptopyrrole: its
5-OH-2-lactam, a product of pyrrolooxygenase.
Report to the Psychiatric Research Meeting of the
Saskatchewan Psychiatric Association. 1973; 46-67.
7. Irvine DG, Bayne W, Miyashita H, et al: Identification of kryptopyrrole in human urine and its
relation to psychosis. Nature, 1969;224:811-813.
8. Sohler A, Beck R, Noval JJ: Mauve factor reidentified as 2.4-dimethyl-3-ethyl pyrroleand its
sedative effect on the CNS. Nature, 1970; 228:
1318-1320.
9. Irvine DG, Wetrerberg L: Kryptopyrrole-like
substance in acute intermittent porphyria. Lancet,
1972; 1201.
10. Irvine DG, Wilson DL: Oxidized monopyrroles
in porphyric disorders and related conditions. In:
Doss, M. editor. Porphyrins in Human Diseases. 1st.
Int. Porphyrin Meet. Frieburg/Br. Basel: Karger.
1976; 217-224
11. Hoffer A: Malvaria, schizophrenia and the HOD
test. Int J Neuropsychiatry, 1965; 2: 175-178.
12. Pfeiffer CC, Iliev V: Pyroluria, urinary mauve factor
causes double deficiency of B6 and zinc in schizophrenics. Fed Am Soc Exp Biol, 1973; 32: 276.
13. Pfeiffer CC, Sohler A, Jenney EH: Treatment
of pyroluric schizophrenia (malvaria) with large
doses of pyridoxine and a dietary supplement of
zinc. J Appl Nutr, 1974; 26: 21-28.
14. Irvine DG: Kryptopyrrole and other monopyrroles in molecular neurobiology. Int Rev Neurobiol, 1974; 16: 145-182.
15. Sohler A, Holsztynska MS, Pfeiffer CC: A rapid
screening test for pyroluria; useful indistinguishing a schizophrenic population. J Orthomolec Psychiatr, 1974; 3: 273-279.
16. Jackson JA, Riordan HD, Neathery S: Vitamin,
blood lead, and urine pyrrole levels in Down syndrome. Am Clin Lab, 1990; 1: 8-9.
17. Sohler A, Renz RH, Smith S, et al: Significance
of hydroxyskatole and mauve factor excretion in
schizophrenia. Int J Neuropsychiatry, 1967; 3: 327-
331.
18. McGinnis WR, Audhya T, Walsh, et al: Discerning the mauve factor, Part 1. Altern Ther Health
Med, 2008: 14: 46-62.
19. Mikirova NA, Casciari JJ, Hunninghake RE:
The orthomolecular correction of metabolic imbalances found in attention deficit hyperactivity
disorder: a retrospective analysis in an outpatient
clinic. J Orthomol Med, 2013; 28: 1-10. 1