Mistletoe in Medicine
 Mistletoe in Medicine
Mistletoe in Medicine
Mistletoe has been used for the treatment of cancer since 1917. This article will describe several different methods of using mistletoe.We will cover the most aggressive therapy down to supportive therapy and then mention special uses of mistletoe, including bladder instillation for bladder cancer, as well as other therapeutic approaches of interest. Scientific literature exists on most of these approaches, and I will attempt to sketch the supporting studies. This does not serve as individual direction for patients, only as information for a better understanding of different approaches with mistletoe.
Heat Seeking Mistletoe Therapy
This approach is used in several European centers, such as the Oeschelbronn clinic, as well as Humanizing Medicine. Very high dose, high lectin content mistletoe, usually from the ash tree, is first infused intravenously daily over several days. This loads the body with high levels of lectins, but the intravenous dosing does not yet activate the dendritic cells. Dendritic cells are special immune cells that can activate and direct the cancer-killing T cells of the immune system. A very high dose below the skin (subcutaneously) is then administered. This is where the dendritic cells live, and they are activated especially strongly (1). A fever of over 102oF is often noted. Like a healthy fever, this process is self-regulated by the body. Patients need to have some reserve of vitality and be able to tolerate several days of fever, often with chills, body aches, and feelings of malaise, usually over 2 weeks. But these fevers often hold an emotionally transformative power. Many of my patients have described lucid dreams. One patient had always had sleep disturbed by anxiety, but had a lucid and peaceful experience of frankly speaking to her breast cancer, telling it that it has served its purpose, and it may go now. This was accompanied by a regression of the tumor.
This Heat Seeking Mistletoe therapy (also known as MFIT- Mistletoe Fever Induction Therapy), as well as high-dose intravenous therapy, has been the method most often associated with spontaneous remissions. Dr Maurice Orange reports on using this method and noting complete remissions from several cancers (2). This case series, included in a dissertation on mistletoe, includes patients who used only mistletoe to treat their cancers (excluding chemotherapy and often surgery) (3).
The Heat Seeking Mistletoe protocol will commonly give symptoms of short-term, local inflammation where the tumor is located. Patients treated at Humanizing Medicine have reported such symptoms during the induction phase. A patient with cancerous tumors in her lungs from stage 4 breast cancer reported a non-productive cough. Chest x-ray was negative for pneumonia or other concerning processes. Several weeks later, a chest CT scan showed her tumors had shrunk to less than half their size. Another patient had metastasis from colon cancer in her spine and liver. She had an achy pain in her right abdomen where her liver was, as well as similar pain in her spine and in her lower abdomen where her primary tumor was located. This occurred the day after her first treatment and corresponded with a robust remission that baffled her conventionally trained oncologist. These body pains are typically temporary, and they represent an immune reaction to the tumor. Immune identification results in a robust attack against the tumor and changes the extracellular matrix (the body’s terrain) to resist further growth or metastasis.
One picture of cancer therapy is the untying of a series of knots. Usually, one needs to gently loosen from many angles these knots. Similarly, with cancer, we should work from many sides- working on not only the tumor, but diet, removing toxins from the environment, decreasing (long-term) inflammation, emotional and spiritual, artistic, biographical, and socially. The Heat Seeking Mistletoe protocol is a strong initial approach in this process, usually reserved for turning the tide when strong measures are needed. Acute inflammation is used to resolve chronic inflammation in the same way that a febrile state may resolve some chronic conditions.
High Dose Intravenous Mistletoe Therapy
The High Dose Mistletoe protocols are another strong way of working with cancer. High doses of mistletoe are infused intravenously. Two commonly used brands of mistletoe are Helixor and Abnoba. Fermented mistletoe preparations are generally always avoided in intravenous use due to the higher risk of allergic reaction, which is quite low with Helixor and Abnoba. Intravenous protocols with Helixor usually start with 50 to 100mg and will use either A, M, or P (Fir, Apple, or Pine). A similar regimen is used with Abnoba products, but at doses of 60 to 200mg, as abnoba has much more fever-producing lectins than Helixor. As the subcutaneous injections are not immediately performed and the dendritic cells are not stimulated, there typically are not high fevers or flu-like symptoms, though these occur occasionally. The infusion dose is doubled each infusion until 800mg Helixor dose is reached or until any of the fever effects are reached. After this induction, infusions are continued regularly, from weekly to once a month. Other methods are to transition to a high-dose subcutaneous administration.
 PET Scan of a patient with widely metastatic colon cancer prior to High Dose Mistletoe treatment at Humanizing Medicine.
PET Scan of a patient with widely metastatic colon cancer prior to High Dose Mistletoe treatment at Humanizing Medicine.
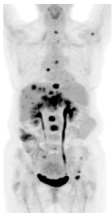 PET Scan of the same patient 6 months after High Dose Mistletoe. Note: near complete resolution of tumor in liver and lungs.
PET Scan of the same patient 6 months after High Dose Mistletoe. Note: near complete resolution of tumor in liver and lungs.
All infusions are targeted to last 2-3 hours. Shorter infusion times can give a patient an itchy rash that is medically classified as a pseudo-allergic reaction. This reaction is not anaphylaxis as it does not lead to problems with breathing or too low blood pressure. It is self-limiting and improves with medicines like Benadryl. I have only seen this reaction rarely so far in short infusions, and it has always been possible to continue mistletoe without a repeat reaction. Review of data from 69 human studies and dozens of animal trials has shown that high-dose Mistletoe is generally safe in the prescribed doses. (4) Most patients getting high-dose mistletoe had fewer incidences of infections during the duration of treatment. Out of millions of doses of mistletoe that has been administered, only a small handful of documented severe life-threatening allergies (anaphylaxis) have been reported (5). No deaths have occurred. It is essential that intravenous administration is performed with at least a rudimentary kit to handle possible anaphylaxis. I have yet to see a case of anaphylaxis caused by mistletoe.
High-dose Mistletoe is often safely used side by side with chemotherapy treatments. Patients report a higher quality of life with fewer side effects during treatment. In one trial, the arm of patients not using mistletoe had a 60% rate of cancer-related fatigue. In the arm using mistletoe, this rate was only 8.8%. Both arms were receiving chemotherapy (6). Another study showed that Global Health status (a measure of overall quality of life) was increased during chemotherapy compared to controls. Diarrhea was 7% versus the non-mistletoe group at 50%. The white blood cell count was increased significantly compared to controls (7). Another qualitative study on the effects on quality of life in cancer showed that mistletoe helped bring about real improvements in patients’ individual biography. “Concrete personal achievements such as changes in the private and/or in the professional environment were spontaneously mentioned by the patients.”(8). Another study on intravenous use of mistletoe for cancer concluded similar results. “The doctors reported long-term disease stability and improvements in patients’ general condition, vitality, strength, thermal comfort, appetite, sleep, pain from bone metastases, dyspnea in pulmonary lymphangitis carcinomatosa, fatigue, and cachexia; chemotherapy was better tolerated. Also, patients’ emotional and mental condition was reported to have improved.” (9)
High Dose Subcutaneous Mistletoe Therapy
Mistletoe can be given in high doses with injections very similar to how insulin is administered. On the extreme side, with the Heat Seeking Treatment, this is done at elevated doses after intravenous loading and can result in an area of redness 8 to 10 inches across or more. These robust immune reactions are often quite sore and very ho,t and inflamed. They can bruise and take time to go down; patients have associated high fevers that many experts have deemed essential for fighting cancer (10). This extreme approach is used during induction therapy to stimulate the dendritic cells and natural killer cells as strongly as possible. Inflammation and slight swelling of existing tumors will often occur; the immune system will cause acute local inflammation. This response is a heartening sign of future responses. The regular monitoring by a provider trained in this approach is essential- in Europe, this is done in a hospital setting. Typically, only people who have not been on mistletoe before will respond strongly to this treatment. Though not every patient is able to manage this approach, it is the most likely to result in strong anticancer results in my experience.
A more moderate high-dose subcutaneous approach is used to transition from high-dose intravenous Mistletoe to home use. I use this approach especially in patients who come from a distance to do their induction therapy intravenously. Usually, Abnoba or Helixor is used, though here the fermented mistletoe product Iscador is also an option. The goal reaction is an area about the size of a quarter to half dollar. Typically, the doses initially used are lower (1-10mg of Helixor, and around 0.2mg Abnoba) but are gradually increased over the weeks to keep the immune response adequate but not overstimulated. Guidelines of every other day injection are the norm, with the iron fast rule to hold off on injections if there is fever (over 100.4F) or if the area is still inflamed. The cost of a month of mistletoe is typically $100-200, though starting out can be substantially less if large-dose ampules are split. Side effects with this approach are usually easily tolerated- slight sweats, mild fevers, usually low grade, and the areas of injection are itchy or mildly tender. Patients report similar quality of life increases with this approach, as well as systematic reviews finding evidence of increased survival (11).
Most integrative oncology experts point to the need for addressing multiple areas of the patient’s domain of existence simultaneously in order to achieve control of cancer. These include addressing the glucose-driven growth of cancer by adopting a ketogenic diet, eliminating toxins (including toxic social issues), and using specific superfoods to address the root causes of cancer (12). I have seen dramatic results with this approach, which uses mistletoe as a cornerstone of therapy. In a remarkable case, a patient with metastatic melanoma with metastasis in the liver declined any treatment except mistletoe. He went into complete remission (13).
Physicians are allowed to prescribe mistletoe in the United States. One issue is liability and malpractice coverage. Personally I feel the best malpractice coverage is a close relationship with the patient and the courage to always do what is right. Low Dose Subcutaneous Mistletoe Therapy Initially, there is little difference between high and low dose subcutaneous mistletoe therapy. Low-dose therapy uses a box of mistletoe called a series that often cycles from a lower dose to a somewhat higher dose and back again. The focus is mainly on staying on the series instead of following the immune response. In High Dose Subcutaneous Mistletoe Therapy the doses of Helixor can eventually reach 400mg per injection. Low Dose Subcutaneous Mistletoe Therapy is given as a traditional approach with mistletoe, or with a palliative goal, or mainly to counter chemotherapy side effects, or for indications other than cancer, such as endometriosis, rheumatoid arthritis, and other issues.
Intratumoral Injection
The case for direct injection of tumors with mistletoe is compelling. Injection of mistletoe into the tumor and surrounding areas delivers viscotoxins, which prompt apoptosis (cell death) of the cancer. Simultaneously, an immune response is called forth by the lectins, which coordinates the display of cancer antigens to the immune system, which may be important for recognition and immune clearance, and thus remission. One case report describes an older man with stage 3c colon cancer initially treated with surgery. When a colonoscopy showed a cancerous polyp, the patient refused surgery but allowed his German physicians to inject this with mistletoe. After the second injection, the patient’s cancer was put into complete remission (14). A pilot trial involving injecting pancreatic cancer with mistletoe through endoscopy has shown promising survival results (15). Two cases of cutaneous B-cell lymphoma went into durable remission after intratumoral injection (16). One of the patients described their treatment experience: During one of the high fevers, an old traumatic experience became disentangled, and I have felt freed up since; I now feel better than before my cancer, physically and emotionally. This type of healing is common after treatment with mistletoe. Mistletoe was injected around the base of a man’s cutaneous squamous cell carcinoma. This was the only treatment, and the cancer disappeared(17).
Intratumoral injections, without a doubt, cause many side effects. These include local swelling of the tumor and surrounding area, redness, and fever. These reactions are thought to hold a critical role in opposing cancer (18). Activation of the lymph nodes associated with the tumor can occur, and this expected and beneficial reaction can cause concern to both patients and oncologists for fear of spreading of the cancer. Typically, this response represents just the opposite- it is the immune system recognizing and fighting the cancer. When I feel that there is a safe route to inject a tumor with mistletoe and a willing and consenting patient, we will tread this path together. Bladder Instillation of Mistletoe. One promising development in the treatment of bladder cancer is the instillation through a catheter of a mistletoe solution into the bladder. This trial showed that mistletoe for bladder cancer was at least equivalent to the use of BCG, without the side effects of BCG (19). A mouse study showed that mice with bladder cancer treated solely with high-dose mistletoe instillation in their bladders had an 82% cure rate vs the controls with only 18% cure. A phase 3 human trial is ongoing. We have had individual patients who had complete eradication of their cancer. Note that this is being looked at as a replacement only for superficial bladder cancer. It is still finishing the investigational phase trials.
Other Applications of Mistletoe
In advanced cancer, fluid can accumulate in the lung or the abdominal cavity. In one comparison study, mistletoe was injected into the lung cavity and was twice as effective as the conventional agent at keeping the fluid from returning to the lungs (60% vs 30%) (20). There have been successful cases of using mistletoe to decrease fluid buildup in the abdominal cavity (malignant ascites) 21 with an impact on disease progression and quality of life of the patient. Especially for children, another less invasive way of administering mistletoe is through a nebulizer machine (commonly used for home breathing treatments for asthma). This can also be a way to treat cancer in the lungs. Older traditional use of mistletoe products, especially in brain cancer , involved taking them by mouth. There has been little evidence that this is helpful, though some anecdotal reports. The concern is that stomach acid destroys the active components of mistletoe. One specialist I know of in Eastern Europe bravely treats brain cancer with MFIT and injections subcutaneously in the back of the neck (this is the lymphatic drainage from the brain).
Conclusion
Mistletoe has a vast role in cancer. Whether it is used as an additional agent for reducing chemotherapy side effects or as the cornerstone of a transformative cancer treatment when no other hope has been given, it stands as the safest, most evidence-based natural treatment for cancer in existence. It is time for this popular European medicine to become adopted around the world.
1) Saha C, Das M, Stephen-Victor E, Friboulet A, Bayry J, Kaveri S. Differential Effects of Viscum album Preparations on the Maturation and Activation of Human Dendritic Cells and CD4+ T Cell
Responses. Molecules. 2016;21(7) 912. doi: 10.3390/molecules21070912
2) Orange M, Lace A, Fonseca MP, Von Laue BH, Geider S, Kienle GS. Durable Regression of Primary Cutaneous B-Cell Lymphoma following Fever-inducing Mistletoe Treatment: Two Case Reports. Global Advances in Health and Medicine. 2012;1(1) 18-25. doi: 10.7453/gahmj.2012.1.1.006
3) Orange M. School of Cancer Sciences, Birmingham UK. Mistletoe Therapy for Cancer Patients. http://www.anthromed.org/UploadedDocuments/0_Dissertation_compressed.pdf. Published
August 2010.
4) Kienle GS, Grugel R, Kiene H. Safety of higher dosages of Viscum album L. in animals and humans – systematic review of immune changes and safety parameters. BMC Complementary and Alternative Medicine. 2011;11(1). doi: 10.1186/1472-6882-11-72
5) Hutt N, Kopferschmitt-Kubler M, Cabalion J, Purohit A, Alt M, Pauli G. Anaphylactic reactions after therapeutic injection of mistletoe (Viscum album L.). Allergol Immunopathol (Madr).
2001;29(5) 201-203. [PubMed]
6) Bock P, Hanisch J, Matthes H, Zänker K. Targeting Inflammation in Cancer-Related-Fatigue: A Rationale for Mistletoe Therapy as Supportive Care in Colorectal Cancer Patients. Inflamm Allergy Drug Targets. 2014;13(2) 105-111. [PMC]
7) Kim K, Yook J, Eisenbraun J, Kim B, Huber R. Quality of life, immunomodulation and safety of adjuvant mistletoe treatment in patients with gastric carcinoma – a randomized, controlled pilot
study. BMC Complement Altern Med. 2012;12 172. [PubMed]
8) Brandenberger M, Simões-Wüst A, Rostock M, Rist L, Saller R. An exploratory study on the quality of life and individual coping of cancer patients during mistletoe therapy. Integr Cancer Ther.
2012;11(2) 90-100. [PubMed]
9) Kienle G, Mussler M, Fuchs D, Kiene H. Intravenous Mistletoe Treatment in Integrative Cancer Care: A Qualitative Study Exploring the Procedures, Concepts, and Observations of Expert Doctors. Evid Based Complement Alternat Med. 2016;2016 4628287. [PubMed]
10) Orange M, Reuter U, Hobohm U. Coley’s Lessons Remembered: Augmenting Mistletoe Therapy. Integr Cancer Ther. 2016;15(4) 502-511. [PubMed]
11) Kienle G, Kiene H. Complementary cancer therapy: a systematic review of prospective clinical trials on anthroposophic mistletoe extracts. Eur J Med Res. 2007;12(3) 103-119. [PubMed]
12) Winters N, Higgins Kelly J. The Metabolic Approach to Cancer: Integrating Deep Nutrition, the Ketogenic Diet, and Nontoxic Bio-Individualized Therapies. Chelsea Green Publishing ; 2017.
13) Kirsch A. Successful treatment of metastatic malignant melanoma with Viscum album extract (Iscador M). J Altern Complement Med. 2007;13(4) 443-445. [PubMed]
14) von S-A, Goyert A, Vagedes J, Kiene H, Merckens H, Kienle G. Disappearance of an advanced adenomatous colon polyp after intratumoural injection with Viscum album (European mistletoe)
extract: a case report. J Gastrointestin Liver Dis. 2014;23(4) 449-452. [PubMed]
15) Schad F, Atxner J, Buchwald D, et al. Intratumoral Mistletoe (Viscum album L) Therapy in Patients With Unresectable Pancreas Carcinoma: A Retrospective Analysis. Integr Cancer Ther.
2014;13(4) 332-340. [PubMed]
16) Orange M, Lace A, Fonseca M, von L, Geider S, Kienle G. Durable Regression of Primary Cutaneous B-Cell Lymphoma Following Fever-inducing Mistletoe Treatment: Two Case Reports.
Glob Adv Health Med. 2012;1(1) 18-25. [PubMed]
17) Werthmann P, Sträter G, Friesland H, Kienle G. Durable response of cutaneous squamous cell carcinoma following high-dose peri-lesional injections of Viscum album extracts–a case report.
Phytomedicine. 2013;20(3-4) 324-327. [PubMed]
18) Steele M, Axtner J, Happe A, Kröz M, Matthes H, Schad F. Use and safety of intratumoral application of European mistletoe (Viscum album L) preparations in Oncology. Integr Cancer Ther.
2015;14(2) 140-148. [PubMed]
19) Elsässer-Beile U, Leiber C, Wetterauer U, et al. Adjuvant intravesical treatment with a standardized mistletoe extract to prevent recurrence of superficial urinary bladder cancer.
Anticancer Res. 2005;25(6C) 4733-4736. [PubMed]
20) Gaafar R, Abdel R, Aboulkasem F, El B. Mistletoe preparation (Viscum Fraxini-2) as palliative treatment for malignant pleural effusion: a feasibility study with comparison to bleomycin.
Ecancermedicalscience. 2014;8 424. [PubMed]
21) Stange R, Jänsch A, Schrag S, et al. [Favourable course of persisting malignant ascites]. Forsch Komplementmed. 2009;16(1) 49-53. [PubMed]